Ruddle Listing
re: "Technique Tips for Locating the MB2"
Oct 2023
Ruddle's Summary Listing of Technique Tips for Locating the MB2
As the holidays approach, many of us take part in festive traditions; in the Opener, Ruddle and Lisette talk about their Christmas caroling cooperation. Then, the two are at the Board, doing a classic clinical Q&A – one important question for each stage of endodontic treatment. After, the questioning continues at the desk; Lisette grills Ruddle on his best and worst of 2025. Season 12 concludes with the 5th Grandkids segment; this time, we meet the youngest, Luca Ostovany, a standout junior tennis competitor with aspirations to play at the professional level. Remember, you saw it here first!
Ruddle's Summary Listing of Technique Tips for Locating the MB2
The goal of endodontic treatment is to prevent or cure, when present, Lesions of Endodontic Origin, at times referred to as apical periodontitis. The role of bacteria in the pathogenesis of endodontic disease is well established, and therefore, it is critical to eradicate these pathogens by employing the highest level of presently developed standards...
For more than 50 years there has been universal agreement that the triad for endodontic success is shaping canals, cleaning in 3 dimensions, and filling root canal systems. Further, it is globally accepted that 3D disinfection is central to success and has traditionally required a well-shaped canal...
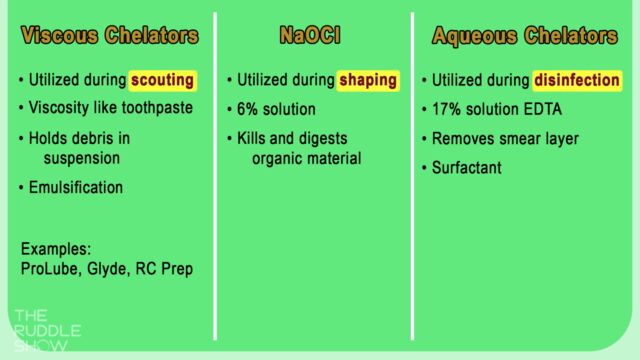
Featured Graphic from The Ruddle Show: Knowing the Difference - Chelator vs Sodium Hypochlorite
Summary Research as presented by Dr. Addison Valdes at the AAE 2024 Meeting (updated graphic by The Ruddle Show)

"The primary cause of endodontic treatment failure is persistent intraradicular infection, reinfection, or persistent extraradicular infection. Intra- and extraradicular biofilms are difficult to control chemically due to the EPS matrix barrier and the spatial heterogeneity of the 3D biofilm structure..."
This transcript is made available by The Ruddle Show in an effort to share opinions and information, and as an added service. Since all show text has been transcribed by a third party, grammatical errors and/or misspellings may occur. As such, we encourage you to listen/watch the show whenever possible and use the transcript for your own general, personal information. Any reproduction of show content (visual, audio or written) is strictly forbidden.
…What would you say is the most surprising or shocking topic for you that you have seen discussed on the AAE Discussion Forum this year?
Do you want me to be brutally honest or kind?
Well hopefully you can be honest and kind at the same time
All right…
Welcome to The Ruddle Show. I’m Lisette and this is my dad, Cliff Ruddle.
How you doing today?
Pretty good, how about you?
I’m doing good and I want to thank everybody out in ‘Ruddlesville’ Land because we appreciate your attendance.
So this is our last show of Season 12, just a heads up, our last Ruddle Show. So we have a big show planned for today. But let’s start off with a little talk about the holidays, because they are fast approaching. So when the holidays come around, no matter what you celebrate, probably you have some traditions in which you participate. For my family, on December 1, we start listening to Christmas carols in the car on every car ride wherever we go. We listen to all kinds of Christmas music: classical Christmas music, then some Christmas music that’s more jazzy or funk in nature. But it doesn’t matter; it has to be Christmas music.
So I know a lot of Christmas songs and lyrics, but I mostly keep my singing confined to the car. I’ve never gone Christmas caroling with a group, house to house singing songs like they did in the past. It was more common to do that in the past. Have you done that ever?
In the past. Yeah, I did it in the past. It was in the late 50s and I was like 9, 10 and 11, and I think we did it three years when we lived in Seattle, Washington. And what we would do is they would – okay, it was a church group and they had the youth. And they would take youth from about my age, I was about at the bottom, and then they’d go up to about 16. They’d break us up into groups, we’d load into cars, and the car had a speaker on top and a tape recorder deck inside the cabin, and as they went slowly down the street we would be let out of the car and we would be running, literally running from door to door, knock, ring the doorbell, whatever, and we’d put out our little can because we were gathering income money for the church and doing good at Christmas time for the people who were less fortunate.
So we would do all that, and then we’d come back every night at about 8:00 o’clock – so it was about 6:00 to 8:00 because it’s dark – and they would give us hot chocolate and there were some snacks and the ladies of the church were counting all the money. And then at the end, the grand finale, they would tell us you were here last week and yesterday you were there. Anyway, we did this every single day and it would lead up to Christmas.
And the last two weeks – because we started a month early – the last two weeks they took the speaker off the car, we all piled into the car, they let us out, and we went door to door in groups and we sung. So they would open the door after we rang the doorbell and we would be singing. So I did a lot of lip-syncing in those days.
Okay. Well I do remember that when my kids were pretty little in my old neighborhood, they were maybe like about 8 and10 years old, I remember one night in mid-December, it was the evening, it was already dark, and there was a knock at the door. And I thought well who’s knocking at this time; this is rude. And so I opened the door kind of abruptly because I was a little bit annoyed, and when I opened the door there were over 20 people right on my front lawn all singing Christmas carols.
And my kids immediately ran to the door and were super excited. I actually felt a little awkward. Like you said, you put out a can. I was like, the whole time they were singing I was thinking to myself, am I supposed to tip at the end? And I wasn’t sure; I didn’t see a can. But at the end we just thanked them and they went on to the next house. But I still will always remember that, even to this day, because I was so taken aback and it was just so funny. We were just all three standing there, me and the kids, and they were singing to us it felt like.
So do you have a favorite Christmas carol?
Oh, you know, when you go caroling for three years and you’re that age, like 9-10-11, a lot of those carols got inside me and I find out as an adult during Christmas time, I’m running around whistling, singing, humming, whatever. Maybe O’ Holy Night, secular Jingle Bells, White Christmas; I like a lot of them. I like basically pretty much all the carols; I would say maybe a couple I didn’t. What about you?
Well I really like We Three Kings, that’s one of my favorites. But I tend to prefer more of the jazz versions of these Christmas carols. But I also really like carols with bells, which I recently found out was of Ukrainian origin, so that was interesting to me. I have three albums that I listen to in the car.
That’s gorgeous, incidentally.
Yeah. I actually did not know what the Carol of the Bells was called, and I was for so long trying to find out; what’s the name of that song that they play? And I’m like Siri, what song is this whenever I heard it.
If we would have rehearsed that we would have actually sung it for the rest of the world to see; and endodontic, oral so they could see what it really is. But we didn’t rehearse that.
Well I do have a 3-album set of Christmas songs, and it’s all various artists. But it’s called Santa’s Funk and Soul Christmas, and I really love those and I would maybe recommend those. I do remember going over to your house when I was younger, and you always had Luciano Pavarotti playing, and I do remember him singing O’ Holy Night.
So are there any Christmas carols that you really do not like? I think you mentioned there were a few that you don’t like.
Well there’s one that stands out: Grandma Got Run Over by a Reindeer. That was an ugly title. And then the lyrics were even worse because there was the hoofprint on the forehead and there was the Claus marks on the back. So I thought it was a ridiculous song.
Well I guess singing is good for people, right; it’s good to sing?
Well singing has many, many advantages -- physical and mental health comes to mind immediately. But it brings people together, brings generations together. It respects traditions and keeps them going forward. I think it’s a great time to have good will and cheer and spread that if you can. So yeah, I think with the health benefits you should be singing at the top of your lungs right now.
Okay. Well we have a great show today and it’s all filled with Q&A, so let’s get to it.
All right. So we thought we would finish Season 12 off with a Q&A here. And for this Q&A we’re actually going to cover start to finish endodontics. I’m going to ask you a question about each stage of endodontic treatment, and these are from questions that we’ve gotten over the years. These are questions that you’ve identified as being pretty important. So that’s why we’re going to have one question for each stage of start to finish endodontics. Are you ready?
I’m ready.
Okay, so the first one is related to diagnosis, and here’s the question. “I know you speak a lot about pulpal sensibility testing, otherwise known as vital pulp testing. But if the clinical findings and imaging point to a certain tooth, is vital pulp testing really that necessary?”
I think it is. We like to have two or three things to condemn a tooth endodontically, so we have permission to either say extract the tooth or try to salvage the tooth. So always our job is to do – we would like to place the pulp through the vital pulp testing. We’d like to place the pulp on this continuum that ranges from health to necrosis. And then of course there are reversible conditions. If you get a restoration of a recent filling you’re going to have cold maybe, but it loops back towards a higher state of health. If we get on the wrong side of the line, it’s a progressive march down to gangrene necrosis.
On this side of the line is either extract or do root canal treatment. So I like to do vital pulp testing to put the pulp on a continuum. It would probably have more importance if I showed you a simple case.
This patient presented with two separate, distinct and unrelated problems. They had tremendous heat sensitivity; heat and pressure. And then they had cold sensitivity. And when I say cold, severe cold lingering for over a minute. So this tooth, when we put a rubber dam on it – I wouldn’t have thought to do that normally because we always say pulpless teeth don’t feel hot or cold, there’s no nerves – there was a missed canal. So I have the photos, you might have seen them at other presentations, but when we opened this one up there were three orifices filled with gutta percha, but pus – pus was coming out of an MB2 orifice.
This one when we put cold on it elevated the patient out of the chair.
So one reason to do pulp testing, if you just did films you’d say geez, there’s a definite lesion there; that’s the one we should work on. Oh, it really hurts to percussion so let’s do that. Well that’s exactly what this endodontist in Los Angeles did, and when I saw this lady, this tooth was severe to pressure and heat, and this was cold, and the treatment was you have to end up doing both teeth.
So that’s an example. Just one case doesn’t make a rule or a theorem, but it does start to say we should reproduce the patient’s chief complaint. Pulpless teeth with endodontics will not feel hot or cold, but there are a lot of times adjacent teeth that we can learn more about the patient’s condition.
So I really believe I like to do that; I don’t like to be surprised. This patient was very surprised that there was another tooth. When I had her hold the hand mirror and I put the ice on this tooth, she said that’s it. The heat was over here. So that’s one reason you might want a vital pulp test.
Okay, so it kind of helps to tell more of the story.
Yeah, I think it gives you a more complete story. And then you mentioned something about they have films. Okay, so do you see the lesion? This is a regular periapical film; it’s well-angulated, we can see everything. But if you look back now you might say well, maybe, maybe. But in the axial slice there’s a huge blowout. If you do the sagittal slice there’s a complete invasion; maybe not quite to the pulp yet, but you can begin to see – CBCT shows us things we can’t see on a normal film. And then with the vital testing you can pulp test this tooth right here; it tests normal limits to cold. So that’s an example where cold probably wouldn’t have revealed the problem. Advanced imaging did.
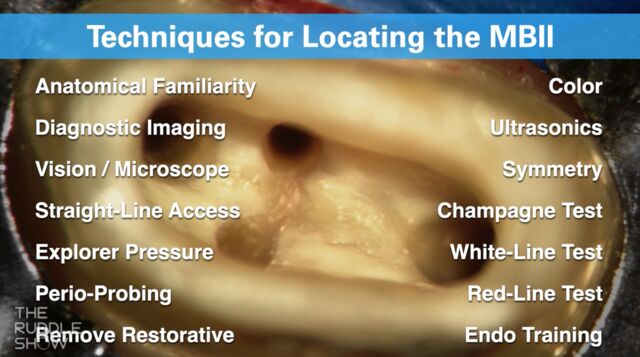
Okay, so the next question is related to access. “I often have trouble finding the canal orifices on the pulpal floor. What are some tips”?
Well what are the tips? The tips are know where the canals are and know your anatomy. Or I should say the old axiom, “know thy anatomy.” But your influence of finding canals is going to be directly influenced by the size of your access cavity. Whether you have microscopes, magnification glasses, loops, transillumination, all that; it’s going to be completely dictated by can you get in there and see. And so when you think that we make them a little bit bigger – this is a Ruddle access that I work with – we’ve got literature to show that it didn’t really reduce the fracture resistance strength of the tooth by having a bigger access. What mostly identifies it is that the fillings go over the marginal ridges.
So basically make a good access would be my first tip, so that you could actually use these kinds of ideas. And I’m not going to read these back to you, but there’s a thing or two I could say about each one. But I just think you need to understand, there’s probably 14 things at least, and I don’t even have two things on this list that I’m thinking of right now that are new since I made the list.
So if you begin to think about all these things and use those things in conjunction with a complete access, you’ll find more orifices.
I think you did a segment on a past Ruddle Show where you went over all of these in more detail, so check out that if you want to know what each one means.
So that’s basically the question – back to that – how do you find canals and what are some of the ideas? Well it’s not just read this list. I had to start with you’d better have a good access.
Okay. The next question is related to glide path management. “I can’t get to length with either my manual or mechanical files. Should I just start shaping with the hope that as I work, maybe the issue will resolve itself”?
Well I always said on stage my whole life: hope is a concept, is a religious idea, it’s in church. You don’t want hope in the operatory, you want reactions and results. So I would have to say this is the question. I’m trying to get to length and I can’t.
Now I’m abusing this file. I want everybody to know, this is not Ruddle working the file like Ruddle would do it; very gently with a breath of fresh air. This is abuse. I’m telling you it won’t move. So what’s the trick? The trick is very simple. Remove canyons of restrictive dentin. Come in here with something like in the Pro-Taper Ultimate family or Pro-Taper Gold you have an SX – auxiliary shaper. And look at how quick this is. I counted last night and I think it’s about 28 seconds. You’ll have the entire body of the canal, the coronal and the middle one-third opened up, not using this any deeper than where the #10 file went. But by just removing canyons of restrictive dentin and flushing it out, guess what? We can take the same file, stick it in the same orifice, and with no other work, slide the instrument to length; and you’ll see it come right out the of the foramen. And it’s hello – there it is!
So one of the tricks if you can’t get to length is pre-enlargement. There’s other one’s too.
Once you’ve pre-enlarged, would you also want to be taking additional radiographs, like for clarification? Like as you’re working until it’s for surely known?
Well when you get to this point – and I’m obviously on the bench with an extracted tooth – you’re either going to take an x-ray to verify your position in the tooth, or you’ll use an electric apex locator.
Okay. All right. So there’s nothing wrong. Do you need to do extra communication with the patient before you start? Like I’m not actually getting this file all the way to length, so I’m just going to start shaping? Or would some people maybe at that point refer? I don’t know. How common is it to actually start work a little bit, not 100% sure, but then as you work along it becomes more clear? Is that fairly common?
That happens a lot. Because there’s the world we see and there’s the world that is. So if you take an x-ray, that has its limitations. If you do CBCT that’s better, 3D. A lot of times that’s great information, it’s useful. But when you sit there chairside you encounter things that you don’t encounter on a film. So imaging is useful, but a lot of times you can work through things as they go. So I wouldn’t chide a doctor who said Cliff, I was trying to get to length, I couldn’t; can I refer it? Because I got a lot of cases referred that way.
So I said maybe your reach exceeds your grasp; try the case. Get better at your communication, pave your way with words, but go ahead and start because a lot of times when you think you can’t, you can. And I’m only showing this to show the importance of glide path.
While we were visiting, the audience saw a file moving in and out, you could push it with your nose, it was a smooth, reproduceable glide path. And if you have glide path, you can shape, you can irrigate and you can pack.
Okay. The next question is related to shaping. “Should I really be making an effort to create smaller shapes to better respect the concept of MIE, and considering there is technology that exists today that can clean these minimally prepared canals”?
Okay. the best way to do this is not try to draw a file and put numbers by it. Just to show you quickly, this is ProTaper. This is a regressive taper. This was launched in 2001. So about minimally invasive endodontics, we were already respecting it 25 years ago.
So if you look at that same file and it doesn’t have a regressive; it has a fixed taper, you can compare. Look at this: 1.5 compared to about 1; 1.2 compared to about 9; 90 compared to about 80. It’s a massive difference, and that is minimally invasive. But we don’t give up our deep shape. We don’t give up our deep shape because the front end is basically the same.
So let’s look at this, minimally invasive. So we’re going to get great shape up here, great deep shape. When can you pack? When you can fit the cone. When can you fit the cone? When you’ve got the shape. So we’re not disinfected, we still have pulp in here, but look at what we can do. We can have a smaller body like I just showed you, still get the deep shape, and then deep shape will give us many advantages.
So you have three finishers. These only work primarily in their apical thirds. So basically deep shape is going to allow you what? Boom! Greater fluid volume. If you look down here, a 25/08 compared to a 25/06, just compare them; there’s 19% more volume in an 8% prepared canal than a 6% tapered canal if we freeze all the other variables.
So deep shape is where most of the anatomy is. Other examples of advantages? You have better exchange dynamics if you’re using active irrigation. You’re going to have containment of your fluid, you’ll have less accidents if you have taper in the apical third, still keeping your body small. And then finally you’re going to be able to have better controlled 3D obturation. I keep showing you a few cases because it’s all about deep shape and having lots of reagent down there, and you can still have a pretty minimally prepared canal in the body.
But to answer it back... 15/04, 20/06, to me they’re underprepared. There’s an abundance of literature that shows they’re not clean. So you might be able to fit a cone and it looks good on a radiograph, and probably a lot of them do heal, don’t they?
So maybe some of these technologies that are claiming they can clean very minimally prepared canals, the research is now showing that maybe they’re not as clean as you would want?
That’s true. We have plenty of evidence that shows that. We have plenty of evidence that shows that. I mean Gary Carr has done this work, Schwartz out of Texas has reported this, it’s been on the AAE Discussion Forum. So it’s not just Ruddle mouthing off. There’s plenty of teeth that were extracted from the mouth, sent to a laboratory, sectioned, histologically prepared, and they showed sheets and loss of tissue in the fins and eccentricities off the rounder part of the canal, with GentleWave as an example.
And then I guess there’s also the issue of you’re going to have to fill these minimally prepared canals.
That’s a technical problem.
So you’re going to have to keep that in mind too if you plan to use warm gutta percha?
Did you hear what she said? Start with the end in mind. So you can make a skinny shape, and a lot of you are going how am I going to fill it? Well that conversation was probably 8 years ago, because everybody started making small shapes and they did go how am I going to fill it?
How are you going to fill it? Well they then discovered single cone and they made whole new methods of obturation that really don’t seal like warm gutta percha.
Okay. Moving on now to irrigation. Which we are kind of seeing that actually we are talking about irrigation while we’re talking about shaping, while we’re talking about obturation. So we’re kind of isolating them in separate steps, but they all affect each other is what we’re seeing.
Are you saying there’s a triad?
I’m saying that each step influences other steps.
They are totally interrelated. They all live together.
Okay, so irrigation. “There are so many new and improved irrigants available today – Qmix, MTAD, Chlorhexidine to give some examples. What is your opinion of these”?
I’ve never used them. So that’s not my opinion is it; that’s just a statement. My opinion is why do I need Chlorhexidine? The biproduct of Chlorhexidine in a root canal space has been reported repeatedly in literature. If you don’t like it, Google it and look for Para-chloroaniline. That is a biproduct of CHX, Chlorhexidine. That’s a carcinogenic; it’s a salt. So it tends to block anatomy, it’s a carcinogen. Why don’t I ever do that? It’s even been reported to cause teeth to discolor. So no, I don’t need it because I can already do everything it says it does.
Mineral trioxide, MTAD. That’s a mixture of Tetracycline and a detergent, I believe, something like that; never used it. If you do this stuff on the bench, do research, yeah, you can show big kill factors. But what is wrong with sodium hypochlorite? Nothing lives longer in sodium hypochlorite than 10 seconds on contact. The key word was “contact.” So if you have a shape that allows irrigant to go into that shape, if you can activate it and exchange that irrigant, you can clean into these inaccessible, uninstrumentable spaces.
So there’s just – it’s a money thing for me. I have sodium hypochlorite and 17% EDTA. So sodium hypochlorite takes care of all the organic tissue; the byproduct of shaping is mud. EDTA removes the mud, and so I have everything I need and it’s simple and it’s affordable.
Are these other ones, are they --
So I’ll show you this slide. We’re talking about reagents, and I was saying I don’t care if you have MTAD in here, a mixture of Tetracycline and a detergent. I don’t care if you have Chlorhexidine. Whatever you’re going to do, activate it. That’s the key. So whatever you choose to use, even if it’s gasoline, activate it so you can get it into these anatomical areas, the lateral canals. These are – they hold things off the canal. Here’s the shape over here of ProTaper, here’s the deep look in the apical 2mm. And then you can see, I have a skin over here, but there’s a beautiful, cleaned out, lateral canal that comes off the body of the canal and goes that way.
So to me, I’m only using two things -- sodium hypochlorite and EDTA. That’s it. that’s all I’ve ever needed.
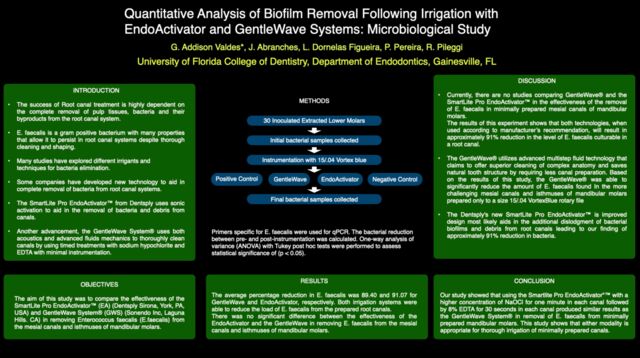
Yeah, you have a lot of things commercially that are for sale. But activate it. Oh, and you have these three things. This is 100K, these are about 100K. If you’re talking everybody; if you’re talking 2940 nanometers. You can get $8-$10-thousand-dollar lasers. They’re not the same wavelength, they’re going to run at about 800 nanometers and they’re not going to irrigate even close to 2940. So that’s about 100, that’s about 100, and this is about 2500.
You can use this, but before you go and grab that or grab your laser, I only want to go right to the results. This was a study done at the University of Gainesville, University of Florida in Gainesville. It was done by Dr. Pileggi, Professor Pileggi, and they showed the reduction of E. faecalis. And the bottom line was this is the EndoActivator; this is GentleWave. And if you read further, the EndoActivator and the GentleWave, they remove from the mesial canals and isthmuses of the mandibular molars. So that’s where they did it on tough teeth, and there was no significant difference between the two technologies.
So I keep hearing about superior. We talked about superior technologies. Are they superior? This is a neutral, peer-reviewed research paper, and this was given at a presentation at the AAE. I just took a grab off of a slide. So you can see that GentleWave was 89, EndoActivator is 91. Well statistically that’s not significant, but we’re a little better. And so the conclusions were quite good.
I see in the conclusions they used EDTA and sodium hypochlorite. Not these other things.
Okay. I wasn’t going to do this, but you got me started. We would never advocate this kind of a shape in my world. So I’m saying the EndoActivator worked in a15/04 hole. That’s crazy! I didn’t even think it would work. That’s the method; that’s the methodology.
The other thing is backwards. You always – okay. They did sodium hypochlorite for one minute, and then they followed – the key word is “followed by” 8% EDTA for 30 seconds. I’ll get this off so you can see it. You always use EDTA first, not second. EDTA takes off the smear layer; EDTA opens up the lateral anatomy; EDTA allows your sodium hypochlorite to penetrate where it couldn’t go. So this was something I would say didn’t follow the protocol. This didn’t follow the EndoActivator protocol that is well-known. And even with all those issues, it’s about the same technology.
So to summarize it for me, there’s lots of reagents; you don’t need all of them, you just need a couple. I’ve said them. And I think the main thing is agitate them. And I got into a little sidebar with agitation, because you can do really expensive stuff or you can do cheaper stuff.
Look. Lasers, I’m not condemning lasers. Because lasers have multiple applications beyond disinfection. That could be an excuse or reason to buy a $100,000 technology. GentleWave is a one-horse pony; it disinfects.
Okay. I just brought that up because I noticed that in this study they used the EDTA and sodium hypochlorite, not any of these other ones like the QMix.
That’s right.
So now on to obturation. “My obturation technique is warm vertical condensation, but I am not seeing nearly as much lateral anatomy as I would like. Why do you think this is and what are some tips”?
Okay. This is from – I consider him a friend and I never shook his hand. His name is Dino Hošnjak, he’s from Croatia. Dino! It’s Ruddle here answering your question live. I’d like to go to Croatia. Have you seen where it is? It’s just across from Italy, must have beautiful beaches and stuff.
Anyway, you said that you’d like to see more anatomy and could it be something to do with obturation. Like Lisette’s been saying, the triad, the shaping, the disinfection, the filling, it all goes together. So here we go real quick.
So I’m trying to go down the canal. We’ve already talked about this in pre-enlargement. I can’t go any further, it’s just blocked. If you looked over here you’d kind of say yeah, I see a system coming down to about here, but I can’t see it after that. So one of the tricks that we’ve talked about is what? Pre-enlargement. Notice how there’s more space in here than you can see here; here the dentin is right up against the file. No matter where you look that file is really – I don’t know if it’s binding but it’s snug, it’s snug.
So just by getting this thing opened up I can put a little curve on the file – listen carefully. I can pass the pre-curved file through the pre-enlarged canal. It will ride in the obstructed area, curve, and now I can begin to feel. Now I can explore that and I can explore the other branch that’s more apical. And we’ll just keep going Dino.
So I can now fit a cone quite easily, just fit one cone, get on that with heat and pressure, downpack right into the apical third, out with the anatomy, and there’s the post-operative film.
So I sometimes don’t see enough anatomy on post-operative films. You’re thinking maybe it’s my obturation. It’s logical to think it would be obturation. But from what we’ve learned from Lisette and what I’ve been preaching for my whole career is it’s not just as simple as the obturation. A lot of the anatomy is blocked on the first or second file. I will do this just quickly.
If you try to move a tapered file, so this is a tapered file and you’re trying to move it down, it’s cutting dentin. There’s pulp in here, so you have a cocktail. You have a cocktail of dentin, pulp, debris, bacteria. You’re pushing that debris laterally into the uninstrumentable portions of the canal, into the dentinal tubules, into the lateral anatomy. So you’re thinking maybe it’s obturation, but as we just saw maybe it has more to do with what? Going back a couple steps and having that shape right so you can flood this thing with reagent, exchange that reagent, and now you have a chance to fill an anatomy.
You know we can stop right here if you want to, because we were going to do resto. Our questions were start to finish endodontics; resto is not.
Well I think our question kind of is the end of endodontics.
All right, then we’ll do a little bit more.
So just to close out on this question. If you’re not seeing lateral anatomy, maybe your problem is not that you need to press harder with your plugger to try to really force the gutta percha into the lateral anatomy. It might actually be a shaping issue where you blocked it when you were shaping and you never cleared it.
That’s exactly right. And so don’t go to single cone, don’t change your sealer, don’t panic. In other words, a lot of times something doesn’t happen in life, like you just said, you’re thinking it’s a packing deal. A lot of people will dance to a new technique because they think oh, this one will be better.
So would you be irrigating more often, like after every file do you irrigate? Is that how it goes?
I irrigate after every file and I dump a 3cc syringe, but I didn’t want to get that technical. I think the main thing is get this thing opened up, get the dentin out of the way and now you have a big reservoir here that’s flooding the root canal system, and that can start to work laterally.
So maybe with better irrigation, then you might see more lateral anatomy.
Yeah, and to get to better irrigation, shape earlier.
Okay, so the last question. “I just finished endodontic treatment and I’m sending the patient back to the GP for a crown. (This is from an endodontist.) What steps do you recommend I take to protect my work, satisfy the patient, but also not infringe on the GP’s restorative plan”?
So what she’s talking about is early on we’ve done segments, whose job is it? Will to me there’s a massive blowout, carious lesion. And we can sit here and scratch our head all day, but at some point somebody’s got to go in here, take out the filling, clean out all the caries and see what’s left. And right here you’ll see there’s a little pulpal exposure, there’s a little bit of hemorrhage, just a little nick into the chamber. Maybe Beth Damas would say do a pulp cap; maybe I would say today do a pulp cap. Because they’re totally asymptomatic, it was normal limits to cold.
But in that day when I saw the pulp it meant endodontics, so we went ahead and did a Wizard Wedge, put a band around the tooth. And we want to build these teeth up so I can go back through the tooth, you can see kind of a swath through here that I’ve made, you can see another swath I think kind of in here.
So I’ve built my tooth up, I have a nice full tooth. Now I can isolate. Now I have reference points because I have an occlusal table, now I have a chamber to hold reagent, and now I can go ahead and do the MB 1 & 2. Notice the curvatures here, it’s quite fun, anatomy going this way, anatomy going that way in the palatal. But I think it’s huge pre-treatment. So that’s one of my -
But yet you started doing the buildup pre-treatment.
Yes.
Whereas I think there’s still probably a lot of clinicians that don’t do a buildup pre-treatment, and then maybe at the end they think I need to do a buildup to send it back to the GP?
Yes. What she’s saying is a lot of you will put cotton rolls up in the vestibule. Okay, my producer is going to ask again, but there was a Scandinavian paper, we don’t even have to go to Scandinavia. I asked an audience live in Los Angeles, I had 1500 people in the room, it was the Western Dental Society. And I asked the audience, how many of you are using a rubber dam? I have a whole story, I’ll just go to the end. About 50% of the room were using routinely a rubber dam. So when I say a cotton roll up in the vestibule to block saliva, maybe some gauzes and stuff, they’re doing – they’re fighting the whole way, saliva is getting into the tooth they’re working on, blood from the tooth is pouring out. People go I’ve got a taste like Clorox, and you go it’s much like Clorox (that’s a joke).
Anyway, then they get all done with the endodontics and I think they’ve compromised. Then they clean everything out and they do a wonderful buildup and put a beautiful crown on it. So I would just say get to it a little earlier and make life easier and more predictable.
I know I’ve heard you talk about that you used to put a cotton pellet in and then send it back. But that became more of a problem because then you were finding cotton pellets that were under the restoration.
Oh, after treatment.
Yeah. So I think the question maybe is also do a buildup, but then how do you seal it off? Because maybe you need to actually call and say do you plan to put a post or not?
Well you’re bringing up many issues. Communication comes to mind; know the referral. So you know what the referral wants, you and him have agreed, you and her have agreed on how you will leave the case for them. But you notice there is no cotton pellet in here. But yes, for years we put a cotton pellet in post-treatment, so when they got referred back you would drill in here, your bur would wrap up in the pellet. It was a convenience; it was a courtesy for the general dentist. But as Lisette said, we saw cotton pellets a lot of times on post-operative films, so that was like a wick or a sponge in there; we didn’t like it.
So we started taking advantage and a lot of times – I didn’t do it in this case, but a lot of times I’ll stub like an MTA type-material over these orifices, I’ll backpack just a little bit shorter, I’ll stub a little material in here. Then I’ll put a different material in here to build that up, and then the new crown, and that’s what Ruddle calls the triple seal. The triple seal.
Okay, so two things. The seal is pretty important to protect your work, so that’s why you’re emphasizing send it back totally sealed.
Um-hmm.
But then also doing a buildup kind of, you’ve told me before in the past that if you can do a buildup, probably the tooth is restorable. So that saves the whole thing of you just did endodontics and the tooth isn’t even restorable.
That’s a huge point. That’s very good.
So two things, the buildup and the seal.
If we did it first we wouldn’t have the dilemma, and you probably don’t even think this would ever happen. It happens routinely all over the world. The endodontist will do some kind of procedure, let’s say endodontics, send it back and they’ll say it’s not restorable. I’m going to know that up front.
All right. Well that’s the questions, start to finish endodontics, and now we’re going to move over to the desk. We going to continue this Q&A, but it’s going to be about not stuff so clinical that you’re doing, but more about the other aspects of our show: a Q&A about community, lifestyle and innovation.
Well let’s go do that!
Let’s do some more Q&A.
Okay, so hopefully most of you enjoyed that clinical Q&A that we just did at the board. Now we’re going to have for this Q&A, as you can see from the graphic, more of a lifestyle, community and innovation focus. This is kind of just you reflecting back on the year since it’s coming to a close soon. So are you ready for this Q&A?
Set to go.
Okay, so what would you say is the most surprising or shocking topic for you that you have seen discussed on the AAE Discussion Forum this year?
Do you want me to be brutally honest or kind?
Well hopefully you can be honest and kind at the same time.
All right. You know, we all have failures so that’s a given. I have failures, you have failures. I don’t know, did you [to Lisette] ever have an endodontic failure? She never had an endodontic failure.
So failures are part of the game, but what bothered me with this case is this is perhaps self-anointed, the number one clinician who contributes on a daily basis a lot of cases. So he showed a case that he treated; it was a mandibular molar and it was the MB root specifically, and he was about 2-3 millimeters short. He could not get to the working length, so he packed the case. I had a little problem with that, because I always think the next day you’re ready to fight and you might get a different outcome; fresh look, new perspective, and from the attitude of I can.
So anyway, he packed the case short and he got one apical portal of exit, the ML. So there was a ML, one portal of exit, short over here 3mm. So the case comes back in two years; there’s a frank lesion where there wasn’t a lesion. And he goes back in and he retreats it. He extends treatment in the MB all the way to length, he packs it and he picks up three additional POEs on one single shape.
So I thought that’s cool. We used to say in dental school, nice recovery. That doesn’t really happen in some offices, because if I’m short, I think I can. And if you think you can, you can; if you think you can’t, you’re right. So that was all fine and the rest of the people started weighing in on this case. And all of a sudden out of nowhere this same guy comes back and he said you know, you know about Nosocomial infections; those are infections that occurred in a healthcare setting, so we give the bugs. And he remembered a guy that came over from London at his study club; he was speaking to the endodontists and he presented a paper that he had published on how to improve prognosis by disinfecting gutta percha points and changing gloves.
So we all change gloves between patients, but some of us change more often. Anyway, the hypothesis was this guy changes them every time he leaves the room, every time he comes back in the room, he changes them before packing, blah-blah-blah; changes gloves a lot during the same single procedure. And in his own self-study he showed that success rates, judged by periapical radiographs, CBCT, before all this song and dance and after the song and dance, his success rates were a little bit better. All of a sudden they were starting to tie these two things together, that maybe our failures are because of gloves.
Listen. I’m sure the chain of sepsis is broken a thousand times every day in a single patient operatory. But I kind of got annoyed that there was some inference that maybe if he would have changed – no, it’s 3mm short. Isn’t that going to trump the glove change?
So I can be kind. It’s normal – it’s not normal. It’s unusual for endodontists not to achieve their desired goals. And when they don’t, it’s a really big person that can go back, free of charge he said, and retreat the tooth. But I always remember the expression: “There’s never time to do it right, but there’s always time to do it over.”
So I didn’t like the attitude, because there’s a lot of young kids that watched that and they go, “Oh gee, this guy can be short 3mm; it must be okay.”
As long as you change your gloves.
As long as you keep changing your gloves and disinfecting your cones. So that kind of rubbed me the wrong way.
Okay. I can kind of understand why, because I had that happen to me before where you see something and it seems pretty clear what the problem is. And then others come in with various other reasons that seem very likely not to be true.
Okay. So what do you think is the most important technology launched in 2025 and why?
Oh, for me it’s very easy, and I’ve used the product. Perimetrics makes the product and it’s the future of damage detection in dentistry. I’ve said this a thousand times. It’s quantitative percussion diagnostics, it’s a cordless handpiece, there’s a little rod, you push a button, bam-bam-bam hits the tooth four times, it goes to the cloud, goes up into a databank of over a million other examinations from around the world literally, because we have people now in Germany. And so it can distinguish between a loose crown that you can’t tell is loose clinically, you cannot tell it’s loose, the patient doesn’t know it’s loose, nobody knows it’s loose. But it can distinguish between a loose crown, maybe the buildup under the crown is broken, maybe the tooth coronally is broken, maybe the post is loose, maybe it’s a radicular fracture.
So through artificial intelligence and deep machine learning, the machine is beginning to look at these various curves because it goes up to the cloud and there’s a characteristic curve. And a perfect bell curve means everything is solid; if you get double peaks you know immediately that there’s something wrong, and this is before you even touch the patient. And it’ll see the unseen. So it will see what radiographs or CBCT would never show us.
So I think it’s exciting, it’s a tremendous diagnostic tool – oh, it’s very good – everybody will probably be talking about this in 2026. You heard it here first.
Yeah. I think that if you’re a regular viewer of The Ruddle Show and the podcast, probably you could have guessed how you were going to answer that question. I actually put in parentheses after I wrote the question for you what your answer was going to be.
Yeah, you fed me right into it.
So yeah, I think that maybe Innerview might be mentioned on every Ruddle Show and every podcast. I think it might come up; I wouldn’t be surprised if it came up every time.
I want to acknowledge Cherilyn Sheets, the inventor, the prosthodontist from Newport Beach, California. And this will be a beautiful year, this coming year, because we’ve got the 5/10K, all the patents, 60 or 70-something patents. It’s worked its way into implantitis and implant people love it, general dentists love it, endodontists are going to adore it.
Okay. Next question. “We often emphasize the idea that an educator is always learning and the importance of being a continuous student for life. So what are some things you personally have learned this year”?
Oh wow! I’ve learned an enormous amount, because the scripts start the journey. Well first there’s a big discussion on the script, and then she makes the script beautifully. And then we follow the script with ideas I have.
Anyway, I’ve learned a lot because I have to do research for the shows; sometimes I don’t know things. But I really like the idea of the X-Nav. I won’t really go into it. It came out to help you XYZ, treatment plan with your CBCT, oral scanners; you feed this stuff into the X-Nav and it’ll line you up, XYZ, for calcified canals. Which I could tell you, it was used on me and I went to school on it.
So I was very grateful for the technology to find what were non-existent canals. I liked – well CBCT is a great technology. Resorptions: you know we talk a lot on the Forum about resorptions; we all encounter resorptions and they never seem to hurt until they perforate, right? So I learned even more about it, even though I practiced for about 50 years.
Some of what you have learned is actually related to the fact that you have been a patient yourself this year. So you’ve kind of deep dived on some of these things.
The most serious learning is self-learning. I loved Tataryn, Rod up there in Spokane; he was a guest. He talked about sinuses and the interconnections between lesions of endodontic origin and maxillary sinus; it was fascinating. Just take home the message; unilateral sinusitis, about 70% the etiology is endo: 70%. I liked Arnaldo Castellucci; he gave a very standard lecture. But what I thought was good – it wasn’t anything I think I learned – but I thought he gave one of the most cogent descriptions of impedance, and how the electric apex locator actually works. So go back and look at that show and you’ll get some clinical ideas as you better understand resistance.
Finally Jean Wu, prosthodontist with Cherilyn Sheets at Newport Coast Orofacial Institute. She gave a lecture, as everybody knows that watches The Ruddle Show, on papilla management, and it was quite a learning experience. Because I don’t really worry about papillas; I don’t try to clamp papillas with my clamp (that’s a joke). But no, I care about the papillas, but endodontics doesn’t grow papillas. So Jean showed us how we can manage it through a variety of different methods.
Yeah, The Ruddle Show guests we have always help us maybe see new information, or information in different ways that maybe is new.
Absolutely.
Okay, so if you were still practicing today, what game-changing technology would you want to most invest in for next year?
In no particular order, if I didn’t have these I would want a 2940 laser. I didn’t just say a desktop laser; there’s 8-10 thousand, we just saw that. We have 2940; I would get a laser because it’s not a one-horse pony; it can do a variety of tasks in the endodontic environment. I would get CBCT. I think you can really start to see things that were not observable. Fill it to the bore section; we showed resorption, right; you couldn’t even hardly see it in the periapical. But with a CBCT it was like ta-da! Oh, I think the drums even played.
And then I think you would want to have Innerview.
All right. So now let’s look at some of our Ruddle Show segments.
Maybe the EndoCator, Randy. Randy Cross, Dr. Cross; maybe the EndoCator.
Okay, so talking about our Ruddle Show segments this year. There’s been quite a few lectures you’ve done at the board. What would you say is your favorite board segment?
Well I liked Show 1; it was pretreatment. And I liked it because so much of endodontics – you know they talk in sports, going downhill or you’re going uphill. Going downhill means it’s going your way, you’re in stride, momentum. If you do pretreatment well and set the tooth up, you’re now practicing downhill. So I liked Show 1.
I liked Show 7; that was on intentional replants. Most people, younger dentists have only read about them, so we showed some. And so I thought that was a good thing to show our 100,000+ viewers, because it’s still very viable in the event you’re going to extract anyway.
And then I liked Show 8; I did 3-rooted maxillary bicuspids. I was supposed to pick one; I picked three.
Okay. So what would you say is your favorite Ruddle Show segment that wasn’t at the board this year?
Well you know, can I mention John? Is this where I mention John? Okay, so John West, Dr. John West; he gave a thing about interdisciplinary treatment. I think it was dentistry and philosophy; the interconnections. I thought he just did a great job, and just to say it real quick, he wants you to see it, he wants you to feel it in your gut, and then he wants you to think about it and execute. So he gave some what you would call silly little things, but they’re remarkably powerful. Like the endline was “rock on,” but that’s after he put a rock – you have to go back and watch that show, right? He put a rock in a course attendee’s shoe so he’d remember not to push too hard on the rheostat when he was driving NiTi.
Yeah, so that section was the intersection between dentistry and philosophy and John specifically spoke about the mindset.
That’s right. And then we did an extracurricular activity off campus if you will; we went to Franceschi Park. And I always – having practiced for decades you’re inside your environment – so anytime I can go outside to like a Franceschi Park, see the city, see the islands, see the sky, see the colors, the shades always changing in Santa Barbara. I loved that one.
Yeah. Probably if you think back to your time in school as a kid, like everybody remembers field trips.
Yeah!
They were very memorable.
That’s right.
Okay, so next question. “What is your favorite podcast topic from the past year”?
Oh, my favorite podcast? Oh, I see. Well it was podcast 28, and that was – I’ll just make you watch it. It was #28. No, it was on Headscratchers. And I loved it because it was real world endo. Because you see mysterious things. You see things that don’t add up.
So Headscratchers was about unusual things that happen quite ordinary.
Okay. All right. “What is one of the best articles you read this year”?
[shows article] I’ll read it to you; it’s a long title. But it was from Yanfeng Ren; he’s a professor at the Eastman Institute in Rochester. That’s Rochester, New York, for our international people. And the title was Improving Clinical Success of Root Canal Therapy Through Anatomy Responsive Instrumentation, Energy Enhanced Disinfection, and Bioactive Obturation. And it’s not just a few little pages of the triad. He gives you the names of the products and what they’re doing, and there’s a technical part, there’s a scientific part. And this paper was not published; he made this paper for his residents. So we’ll have this available for you; I got his permission. We heard from him just two days ago; it’s fine to show it. But you might want to glance at it.
Okay. We’ll have that in our show notes. So the last question: “At the end of the show today we have another grandkids’ segments where we will meet your youngest grandson, Luca. And one of the quotes that we say about grandkids here on The Ruddle Show is that the grandchildren restore our zest for life and our faith in humanity. So how have your grandkids inspired you this year”?
Oh wow. I’ll probably say about the same thing for everyone, but if I start with the shooter, that would be called Isaac Kershner who is just back in the control room. Isaac is amazing in that he has a big imagination, he’s extremely curious, and he uses critical thinking. And he makes a lot of stuff; stuff that you would think oh, he bought it somewhere. No, he’s making joints, you know wrists, elbows, they have to articulate; so he’s got to figure out how joints work. He reminds me of Leonardo da Vinci, who studied on the cadavers so he could give anatomy lessons. So Isaac is an amazing kid to me; he inspires me.
Eva. I relate to Eva almost as much as any of the grandchildren, if not the most, because as a professional, she’s in cosmetology, she has patients – oh no, she has clients, sorry. I have patients, you have patients, she has clients. Aren’t they the same? It’s taking care of people. So she has fabulous hand/eye, and so she can make people look their very best, put smiles on faces like you put out pain and it’s joyful. Patients think it’s a miracle, and you say no, it’s ordinary, I do it every day. So Eva is terrific.
Noah. What can I say about Noah? I think he’s the tallest grandkid, and he’s strong, healthy, smart as a – look. He’s on the (Camino) de Santiago, everybody in Europe knows this. He’s taking that pilgrimage out to the sea, it takes several weeks. He’s on his own. He’s got a little knapsack and I’m learning a lot about these – I call them hostels – but where you can come in and stay a night or two, and you can get a breakfast or a dinner. And the photography he’s taking and sending home; I’m really, really proud of him. He’s going to go far, he just doesn’t know yet exactly what he’s going to do, but it’s going to be very special.
And now Sophia. Well this now must be a family contagion, because Noah went on the (Camino) de Santiago; she just came back, Sophie just came back from the Pacific Crest Trail.
That was a four-month expedition.
And that was four months alone in a tent at night. She was carrying like 40 pounds. She started close to Canada; she ended up at the actual border, Mexico/United States. The experiences I can’t go into, but I think her determination, I think her willpower and her can-do attitude is going to serve her well in life.
And then Luca is going to be our guest. Maybe we’ll just keep it short. But Luca is the last kid in, he’s #5, almost ready to catch his brother in height. But he was an amazing soccer player and now he’s an amazing tennis player. And I’ll just say in closing, I’ve had the chance to watch him hit. Because I don’t see him hit. A lot of these tournaments are out of town, they have fly somewhere, I can go on all of those. But I’ve seen him hit at the club here in town against professional people, guys that were on the circuit, and the sound of the ball of the racquet is string music. So he’s an incredible kid.
Okay, yes. And so that’s it for this Q&A, but we’re going to close the show with some questions for Luca, who’s going to be joining us for the grandkids’ segment.
Oh great! Is Luca on the set?
I don’t think so. Maybe he’s going to arrive shortly.
All right.
Okay, well that’s it for this segment, and moving on.
Okay, so we’re joined by a very special guest today, and it’s Luca, who is my nephew and your grandson.
He is.
So you and Mom have five grandkids, and we’ve met so far the other four on The Ruddle Show. We’ve seen – maybe you’ve made some appearances over the years, but you were little then.
But anyway, we’ve seen Noah, Sophia, Isaac and Eva, and now today we have Luca. And the topic today is going to be mostly tennis, right?
Yeah.
Okay, so are you ready for some questions?
Yeah, let’s do it.
Okay, well we’re very happy that you’re here, even if you’re not.
I’m happy to be here.
I wasn’t sure. So the first question is an easy one. How old are you and what is your grade in school?
I’m a 17-year-old, I’m a Junior, and I go to ICL Academy; it’s an online school.
Okay, and that’s to free up some more time for tennis?
Yeah.
Okay. I actually was very surprised when I saw in parentheses that you were 17, because to me you're always going to be Little Luca.
So what keeps you busy day-to-day?
Basically just tennis and school. I’m pretty busy with my training and stuff, and then when I’m not training, I’m trying to catch up on school and everything.
Right. Do you have a lot of work? I mean I don’t know what it’s like to be home schooled, but does that require as much time as regular school? Or would you say a little less time?
Definitely a little less time for sure.
More time for tennis?
Yeah.
Well he probably – you do more than tennis though. Like in training?
Well we’ll maybe get to some other questions. Patience.
So has tennis always been the number one sport for you? Did you always know that you wanted to compete in tennis at a very high level?
In the beginning, I think around 8, 9, 10, 11, 12, I was playing both soccer and tennis. But then around 12, I just chose to stick to tennis because I thought it was more fun as an individual sport.
Well also your older siblings and Isaac and Eva, there was a big tennis focus when you were little. I think Isaac might be 10 years older than you exactly, and he’s the oldest grandson. So there’s a little bit of an age gap, but you saw them playing tennis and maybe you wanted to try that too. And then it turns out you’re better than all of them! Okay, just kidding.
Don’t embarrass him!
Okay, so when did you start competing in tournaments?
I think maybe around age 8-9. Not really too serious, but I was competing in some tournaments locally in Santa Barbara.
Would you say that you were driven to want to be in tournaments? Or were you placed in the tournaments by your parents and you didn’t really want to do it?
No, I was really passionate about tennis and I wanted to compete. But I was also half and half with the soccer as well. But now I definitely take it more seriously than I did before.
Okay. Because I know whenever I tried to sign up Isaac or Eva for a tournament, Eva especially was very against it. You actually happen to have the same birthday as Eva, but she hates tournaments and you love them.
So you’re traveling a lot now for some national tournaments, right?
Yeah.
Where have you been?
I’ve been to Florida a couple of times, I’ve been to Oklahoma, I’ve been to Michigan, and now later this month I’m going to go to Kansas City for another tournament.
And that’s an indoor one, right?
Yeah, indoors. It’s my first one.
So have you played on any indoor courts at all so far?
I’ve probably played like an hour total in my life indoors. But basically no, not really.
I’m wondering. At least you won’t have to worry about the sun in your eyes, but I don’t know the light situation.
Yeah, we’ll see. Hopefully it’s not too dark in there.
Do you prefer singles only, or do you also play doubles?
Well singles is my top priority, but still for the comradery and stuff I like to play doubles; it’s also fun.
Would you say that play doubles helps your singles, and vice versa?
I think a little bit. You also get to be on the court more, so when you’re at a tournament, if you want to get used to the courts and the place and stuff, it’s good to have more time on them.
Do you have a regular doubles partner that you usually play with? Or do you play with different people?
No, I feel like every tournament I’ve played it’s with a different player.
Well at least you’re good enough that other players want to play with you.
Yeah, I guess that’s true.
So what is your current ranking? And I see the answer here that your mom wrote, and I actually was very impressed.
Yeah. I think I’m top 150 in the nation for 18 and under. And in Southern California I’m like top 20.
Well Southern California is one of also the top regions.
Top region, yeah.
So that’s really excellent Luca.
Thank you.
I also hear you are labeled a five-star college recruit. Are you interested in going to college?
I’m not sure yet. I’m just trying to weigh my options and see what the best would be for me. But I’ll most likely take a gap year after high school to give myself more time to choose.
Is there any college or university that stands out to you as you would maybe consider going there if it was available?
Yeah, if I went to college I’d probably want to stay local and go to like UC Santa Barbara, just because it’s like 20 minutes from home.
I think they have a pretty good tennis program there too.
Yeah, it’s getting better for sure.
So back to training. How many hours would you say per day that you’re on the court? Because I know that your training is not only just hitting balls on the court, right?
Yeah, for sure. Probably just on the court though, depending on if I hit it once or twice probably 2-4 hours. Plus the off-court stuff, strength, conditioning, stretching.
And tell us some more about that. Where do you do that?
I do it in the room, like right there.
We have a gym in the studio.
So our studio has a multi-faceted operation, so there is a whole gym back behind the wall there. So yeah, he’s going crazy in there.
But what kinds of cross-training do you do?
A lot of strength training, and a lot of stretching as well to keep my muscles and body health. I’m also starting to do some more conditioning training with sprints and running and stuff like that.
What about any dance? Are you interested in doing dance?
Yeah.
You always hear about athletes that also do dance because of balance and coordination.
Yeah. I haven’t gotten into that. I haven’t thought about it too much.
Your brother did. Noah did.
Yeah, he’s just started doing some dancing. Now recently you actually received a sponsorship, right?
Yeah, I got a sponsorship deal from Yonex for racquets, shoes, clothes, strings.
Did you already use those products?
I used the racquets, but I haven’t used the clothes, shoes and strings. So I’ll probably switch over to those.
What about the shoes? Do you think they’ve been a good pair?
Yeah, I tried them. They’re pretty comfortable. Kind of like Asics that I wear right now.
That’s very neat. So outside of tennis and training, do you have a life? What do you do to keep busy?
Well normally my days are pretty busy when I’m not playing tennis and school and stuff. But I like to go to the beach, go to the movies, and also just hang out with family and stuff.
Okay, here’s a tough question. What is your favorite meal to eat, and your favorite dessert?
Probably pizza; and for dessert maybe like apple pie or something.
Oh, apple pie!
Really? Meme’s apple pie?
Yeah, for sure.
Okay. It’s getting to be that time where she’s going to be making some pies.
Yeah, looking forward to that.
Okay, and then I have this last question here. Where do you see yourself in five years?
Probably either at college or on the pro tour or something. But hopefully tennis at a very high level.
I see myself in five years at Wimbledon watching you play.
Yeah, hopefully I see myself there.
Yeah everyone. Probably you’re looking at the future number one men’s tennis player in the world, so just remember you saw it here first.
Yeah, hopefully.
Well do you have anything else you want to add? Or do you have any questions for Luca?
Well it’s been impressive watching his journey. I remember when he was a little toddler and the racquet was longer than he was. So I’ve kind of just watched it all go along and develop. But like I said earlier before he was here, I got to see him hit a couple times against some pro’s up at the club, and I mentioned the sound off the racquet. So the game has really developed and we’ll see what happens. But the good thing about Luca is he’s not really thinking about that. But of course he’s envisioning it and he’s making a pathway to connect the dots. But he loves the game. And his coach told me one time there were four buckets, all technical stuff, but he said there was this fifth bucket. And I said what’s that bucket? He said it’s the bucket that’s got to be brimming over with love. And Luca loves tennis. I mean he eats, breathes and sleeps it. Nobody has to poke him; he’s ready to go.
Yeah, and just talking with you just briefly before we even started the shoot; it’s impressive just how grounded you seem with everything. And the humility is there too. But you’re really a star.
Thank you.
It’s very inspiring. And we talked about how you were inspiring him and the other grandkids inspiring him all year long. And you inspire me too.
Thank you.
Well I have one thing. He did say something at his graduation from Montessori and I think if it all the time. Would you tell the audience, because it could help an endodontist. It really could.
It’s… “Good, better, best; never let it rest until your good is better and your better is best.”
Okay, excellent. And with that we’ll end Season 12 on than great quote. So thank you.
Thanks Luca.
Thanks for having me.
Yeah, and we’ll see all of you next year on The Ruddle Show.