Okay, all of us that are out there practicing. We encounter occasionally patients that come in with a tooth that’s been initially treated endodontically and it’s failing. So I normally used to say – and most of us do say as teachers – well you could consider retreatment. Well you could consider retreatment, and even if you needed to, you could advance towards a surgical approach. So that was initial treatment: strike one. Strike two was the retreatment, and surgery was three.
But then if that fails and the tooth is still symptomatic, we normally just extract the tooth, don’t we? So what I want you to consider is what if you could extract the tooth and do the corrective work in your hand and replant the tooth?
Now some of you might think this is crazy. What Ruddle is talking about? But there are probably in the literature 6,000 references – 6,000 – to the intentional replantation. There’s probably 600 articles roughly out of that 6,000 that actually talk about it. And there’s very few if you start to look at good papers and good methodology, there’s only a handful of papers that actually describe what I would consider something you could really consider.
So I’d like to just bring this back to the illumination of the international market, because if you’re going to throw it in the wastebasket, maybe you’d like to take a look at it and see if you can do something really cool and then put the tooth back.
We’re not going to have time today to talk about every little step. This is just a concept. Intentional replants are alive and well, and when appropriately selected, they can be viable.
All right. So you have your team and you work with microscopes, you see some failing teeth. But what I want to do is make a little quick flowchart here for you. Teeth fail, so when we’re looking at the cause, the etiology of failure, they fail because we as dentists sometimes not only don’t respect the root anatomy – notice I said the root anatomy – but we don’t sometimes even understand perfectly root canal system anatomy. So root anatomy would be like concavities, fluting, external proximations and grooves; those are the things that sometimes even though it’s on the outside it might influence what we’re doing inside. All right, so root canal systems and the anatomy of the root.
Another thing is deficiencies. Somebody might fill a canal 2mm short, somebody might miss a canal, they didn’t find it in the orifice. Sometimes we don’t see things or because of training we do things a certain way that we would consider appropriate, but it turns out that it might be the difference that made the difference. It might be why it’s failing.
So deficiencies in treatment to me are a complete difference from an iatrogenic event. Running a post out the side of the root, huge shapes that don’t respect external root anatomy – there’s that word again, root anatomy. Those are more like iatrogenics; there’s nobody teaching that anywhere in the world so dentists that are doing that aren’t following any kind of training that was introduced in their programs.
So that’s the cause of failures. I think you could take any failure in the world and put it into one of these buckets. It could even be a fractured tooth because of overzealous preparations, canals that are shaped too big for the roots that hold them, things like that.
Well what do you do? Normally what you do is you assess failure, and you might think – Ruddle almost always thinks I need to go back in the tooth non-surgically. I might see a crack through the axial wall, I might see an extra orifice that wasn’t uncovered. I could use ultrasonics, we talked about Castellucci and we talked about the SINE tips, we talked about buck tips, there’s different ways to refine the access cavity. You might be able to find something that you can address.
And then sometimes you might do the best retreatment in the world, but you inherited something that was very difficult. Your odds were not good that you could overcome the deficiencies in primary treatment or the iatrogenic event, so you’ll go right to surgery. And sometimes some clinicians find the failure and go to surgery immediately; that can be okay. I have learned over the years that it’s better for me to go back in and re-enhance the foundation. So if I am going to surgery I trust what has been done coronal to the surgical work.
But you can do these procedures and you can evaluate them, but what if a fistula persists? What if the symptoms don’t resolve? What if the lesion radiographically appears to be getting larger, not smaller, after treatment? In that case we’re going to extract and normally most dentists will say that’s enough! I’ve had it right up to here, three strikes and you’re out.
But some dentists are thinking outside the box, and based on a lot of factors – and I won’t be able to go through them all today – they might consider taking it out and putting it back in. I guess we could look at a case to get started.
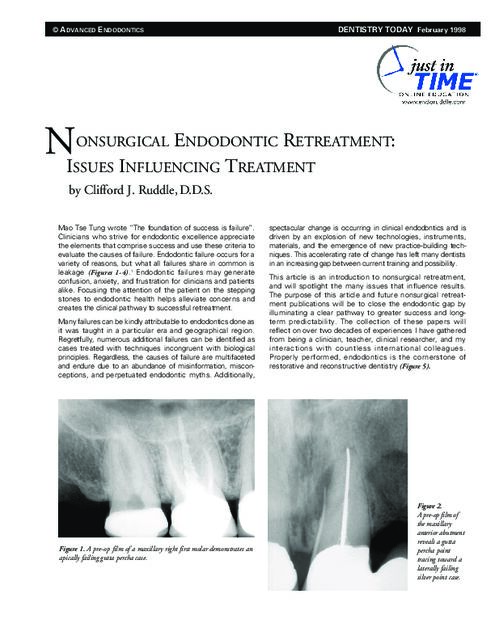
Okay, so let’s look at this, it’s our first case. I’ll show three cases of replantation, intentional replantation. Sometimes things come in and you have to do a series of procedures before you even consider that. In other words, I have a big diffuse lesion in here; it’s wrapping around the apices of several roots associated with different teeth.
And so I’m looking here and I’m thinking boy, this could be a tough access because this crown is kind of sitting like this, but the roots are kind of on a bias like that. So be sure you look at your inclinations. Because if the root is going like this and the crown is like that, and I don’t even see a canal until about right in here. So this could be pretty tricky going through the posterior abutment of a bridge and then picking up the mesial systems. And then I even see something in here that might be resorption. I don’t know what that is. I have a regular canal that goes down to about here, and then I have this diffuse lesion around the distal root. So I’m thinking this root is probably more complicated than maybe its straightness – ha-ha, straightness, right? Straight roots hold hard, curved canals in the apical thirds oftentimes. So that’s kind of what I see.
When I look here I’m looking at endodontics, but it looks like maybe this tooth had surgery, maybe it’s just resorption, but that’s pretty flat. Roots are usually kind of bullet-shaped, kind of bullet-shaped. This one looks a little flat too. The patient doesn’t remember that, but they’ve had a lot of dental work and that’s what they do remember. So it’s possible with shorter roots, kind of blunted roots.
And then I look at the distance from here to here, the distance from here to here, and they’re not the same. So there could be another system in that tooth, but it could be a blocked canal apically, it could have been a transported canal, it could be the ledge that became the rip and the tear.
So I’m seeing that with that tooth, and the patient wants both teeth. This is a second molar, this is a third molar, and lots of times patients want to keep third molars, especially if they’re in occlusion with the opposing tooth.
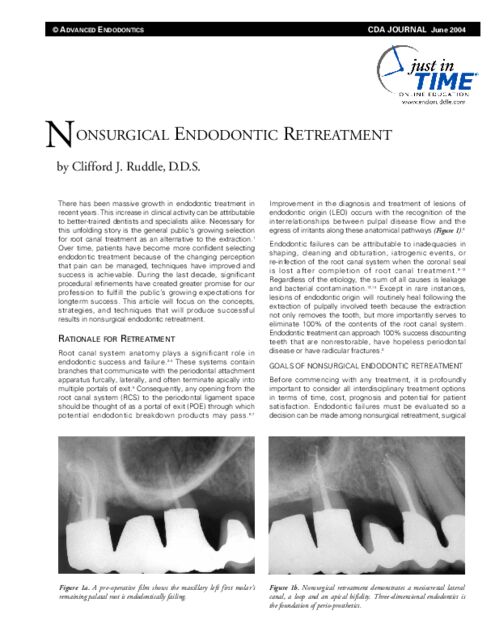
So we go ahead and do one visit. It was a longer appointment because it’s a tough case, long, long roots. But notice the curvature, you can see it right to here, see that canal coming down quite nicely. But then you’ve got a branch here and a branch there, and you can see we got those. And then we’ve got a little furcal canal to what we looked at suspiciously on the preoperative film. As I have gotten older as a clinician, things that I see that might be anatomically related, oftentimes they are. The portals of exit, remember they form adjacent to the lesions of endodontic origin.
So that takes care of that case. But what about that molar? Again, we think it’s transported; we think it’s blunted. The crown/root ratio; if you look at the crown/root ratio, the part above the bone, the part below the bone, it’s about one-to-one. So that’s not real favorable for going back in and doing surgery because of the external oblique ridge. And that makes the shelf, the buccal, shelf, and all of a sudden you’re going to be going through a lot of bone. And don’t forget it’s a third molar and don’t forget as we go posterior, the neurovascular bundle starts to swing up and it gets pretty close to being underneath these roots. So you have those kinds of considerations.
If you’re going to extract the tooth – and when I told the patient all this and I was leading them kind of towards I could make an access and go back in and explore around – the general dentist said no, I don’t think me and the patient want that. So strike one, I can’t do that. I could, but I didn’t have permission. I then could do surgery, but I don’t like the crown/root ratio, as I just said. And finally I said okay; you give me really no more choices, so why don’t we just extract the tooth? And the patient sags in the chair. But what if we could extract the tooth and do corrective work in our hand?
So that led me to this case – it wasn’t the first case I had done, but it was one of the early ones – it led to me doing about 50 intentional replantations over about a 45-year career. So you can see if you do the math, that’s not very many per year. And I lost about 8 or 9 of them, and I had many of them – that’s over 40 left – that went for over a decade, and some of them when I retired the patient still had those teeth.
So it can be a really, really good procedure, but you have to ask yourself: who should do the work? If you’re going to go ahead and extract the tooth, who should do the work? We can talk about – it could be any of these three people on the multi-disciplinary team. I stopped doing them personally because how many extractions does Ruddle do? I work in a complex, I have an oral surgeon within 100 yards. I took him out to dinner and we had a long, pleasant visit -- Dr. Ashamalla. We call him the Egyptian Madman; he could do wonderful things with his hands. And I said look. You’re used to getting in there, boom, and rolling a tooth out fast; and if it breaks you don’t care because you’ll section it and take out the other root. I want the tooth to come out in total. So I said you are way better than I am because you extract teeth every single day, multiple times. But I need atraumatic extraction.
I’ll come back to this at another time and the producer will remind me so I better be careful what I promise. But you have atraumatic techniques, especially if an implant is considered. And you can do vertical extractions so we don’t do so much back and forth, buccal/lingual rotation with our hand and the forceps. We’re doing more of a procedure where it’s like taking a cork out of a bottle. They have different kinds of forceps that can move the tooth more vertically and pull it incrementally right out the socket.
So be aware of the atraumatic, be aware of working with other members on the surgical team. The whole extraoral time we had down to about 5-7 minutes. Most of the literature was 15 minutes; some were 10 minutes. I want to talk just another sentence on the extraoral time. You need to go through the drill with your staff and with the other office, so when the patient’s over there, they’ve been seen on a consultation, they’ve been seen with me on a consultation, all the chit-chat is done. They go over there, the phone rings in our office, and they say Dr. Ashamalla is just about to deliver the tooth. Well guess what? My assistant is standing right there with a cup filled with Hank’s Balanced Salt Solution. It could be bacteriostatic physiological saline solution. But some kind of a cup and some kind of solution or reagent that is conducive to keeping that periodontal ligament and the tissue fragments vital and alive.
So you have that down. They start walking across the complex – not the patient yet, they’re still sitting in the oral surgeon’s office – the assistant’s flying across the complex about 100 yards, and she comes into the office and she’s got the tooth. We’re already there. My other assistant’s there, I’m there, and we’re ready to go to work. And things we might consider doing is having the armamentarium present. So here’s the Hank’s Balanced Salt Solution, it has some calcium, it has some magnesium chloride, it has some materials that are very, very useful to keep tissue alive.
We don’t hold the tooth in the forceps at this point. We grab with a saturated gauze with the reagent. And I want the assistant to have suction and I want this to be flooded with water. I want the tooth wet at all times, and we immediately need a diamond bur, zzzzp, you’ll do your apicoectomy and knock off roots. Sometimes you’re removing the part of the root that has the broken instrument. Sometimes you’re removing the part of the root that was transported or ripped. Sometimes you’re removing the big curve in the root that nobody could get around clinically endodontically. So the roots need to be resected quicky with a tapered diamond, and the debris will be flying around but it’s being flushed off, we have a tray down here to catch it all and we do it right over a bathtub. (If you believe that you’ll believe anything.)
Now you’ve got the roots resected and you’re looking right at them. You can stain them with Methylene Blue, Chinese Red, to just see if any dye is absorbed in other portals of exit. You might even choose to resect a little bit more. Be aware of the crown/root ratio I talked about previously.
This is the Munce Bur. Okay, I better change colors so he doesn’t panic. This is the Munce Bur – Munce, John Munce. I think it’s C. John Munce. So he’s up there in Idaho, he’s up on the mountain, he’s living the good life. This is the Munce Bur half round bur, and I like it because most teeth that have been endodontically treated, the foramens are bigger than a quarter round bur – that would be his next size smaller this way. And so I can do that, but a lot of times if you’re coming around at an angle you can just grab your ultrasonic instrument too. So these two instruments, one’s in a latch-type, slow speed handpiece. One is in a contra-angle generator, an ultrasonic generator behind it to drive it. And you could do these preps laterally, vertically, however you want to do it, but they’re done very effectively and very quickly. Remember -- extra-oral time, the clock is ticking.
So you can place your retro material. It could have been in the old days amalgam, it could have been Super EBA, it could have been bio dentine, it could have been probably not MTA because of all the flushing. I’ll probably flush the MTA right out of it because it has a set consideration at this moment; although I’ve talked to you on this very show that they have MTA coming that can set in 5 minutes, 10 minutes, 15 minutes. You choose the set time you want and then it’s pretty stable and inert; it’s not going to get flushed away rapidly like the current MTA most of us know about.
So you can put your favorite material in there, and then I want you to reach over buccal and lingual with your gloved fingers and squeeze the cortical plate because it’ll flex a little bit from the extraction that was done by the oral surgeon in my case, and that will collapse the plates a little bit. So when you put the tooth in and you push down, oftentimes in molar teeth – I didn’t say single rooted teeth – in molar teeth, they snap back into place. There’s still a lot of mobility, but the tooth won’t just fall out of their mouth. They won’t swallow it, they will not aspirate it, they can go home with it like that. You just have to give them the proper oral instructions about eating and chewing like you would any post-extraction site.
You can splint, and we’ve talked about that on other shows so I won’t really go into that. If you think the tooth is going to fall out, then you’ve got to splint it. But the splints, the bottom line is the splints must be very soft, they should allow for some mobility. We don’t want to lock that tooth down or we’re certainly going to inspire external root resorption. Either replacement resorption, or worse, inflammatory resorption. Even some of those 6, 8, 7 teeth I lost; even when I lost them, I only lost one within 30 days, inflammatory resorption. That’s because I had it bolted down, splinted, immobile. Wrong, go read Andreasen. We’ve talked about Andreasen before in traumatology; he talks a lot about this stuff, the intentional replant. So those are some of the considerations. Splint if you have to, but it’s a softer splint. You can snap them in and most times that’ll hold it.
So if we just fire out and go forward, this is at about 10 years; this is at about a 10-year recall. We’ll get back to something a little better maybe -- 10-year. And you can see the bone is quite nice, the furcation and all this thickened, it’s gone on, the massive lesion, it’s off the film, comes up over here. You can see it’s all grey in here, healing is ideal.
So that’s an example where we kept the tooth and did a 10-minute, a less than 10-minute procedure, and I had the right team. I had the oral surgeon to come across and pick up my deficiencies and my oral surgery skills, so we had the best person to take the tooth out. If the tooth cracks or breaks they’re in the oral surgeon’s office. Who’s better to go after a root tip? You know we talked about prison dentistry earlier where we said one of the few things they refer is third molars. And when they are in the clinic in the prison, BOP, Bureau of Prisons; when they break a root tip, sometimes because of experience they have to refer that case out. So if you have anything break, they’re in the right office; they’re in the office of the oral surgeon.
All right. I’ve shown this case before, but I’m showing it just for fun again. You need to see different ideas and this is an idea where we have a big post. This is a post that’s deviated; you can see it’s deviated in the straight-on angle where we’re basically breaking the contacts perfectly right in here, but a little overlap in here, a little overlap. And you can see when we move the cone a little bit and we come more from the mesial, now we can really see that post is deviating much more than a single image would have ever disclosed.
So I have said for a long time now, take three preoperative views, moving the cone in the horizontal angle up to 30° mesial – you don’t have to go 10, up to 30 – come back to central, straight-on, and go 30° to the distal, and those three views will give you a lot more information. Of course if you have a CBCT you’re going to take that immediately; I still think there’s a benefit of more than a single preoperative digital x-ray.
So we’ve got a sinus tract, massive lesion, previous endodontics, it’s a dentist’s wife. The dentist is always there too; it made it real pleasant. He wanted me to correct the post. I was finally able to convince him this post was a little off axis. He didn’t agree here, he thought it was perfect, never saw bleeding. That doesn’t mean anything does it? Look at the result. Years later, a huge lesion on his wife.
So here a combination flap is coming up. We reflected, you can see the osseous window, we’re taking out a massive wad of granulation tissue that’s in that black lesion radiographically. You can see from kind of a lingual view, we can see the root up in here, we can see a big clump. When you see a big clump – not like tags, but a clump of tissue – remember back to the x-ray; that’s the post and that’s granulation tissue in the bone over the post. We don’t want to scrape roots, we just said that on the previous case. Do not scrape roots, just flood the roots with copious amounts of Hank’s Balanced Salt Solution, keep everything moist, the root moist, the sharpies fibers moist, the granulation tissue moist, and all the tags of tissue; keep them all alive.
So it became clear I could not approach it. I could no approach the defect. It was around the mesial, but worse, it was on the palatal side. And I’m just showing you different views; now you’re looking straight facial. You can see the leakage, you can see the staining of the gutta-percha; so not only was the post out, but that is overt, frank, visual leakage. Notice the black rim around the pink gutta-percha.
And now when I scrape off some of this, some of this, just get it out, then you can see there’s the post perf. This is directly, almost straight lingual. This is the lingual surface, the palatal surface. So there’s no way surgically you can approach this unless you cut the whole root down, and then you might be able to bevel the root a little bit further and get the post tucked back inside the confines of the radicular space. You might be able to do that, but then you don’t have any tooth to replant. So this shows the power of being able to visualize it and do something about it.
So there’s the apical repair, there’s the lateral repair, lateral repair, apical repair. This required a splint. This is a conical shaped root so I told you not splint when they snap back into place. This went back to place easily, but guess what? It started to just kind of creep and drift a little bit incisally; it wanted to come out. So we did have to do a soft splint on the facial just to kind of hold it in there.
And then here we are a little bit later in time and you can see where we had the massive, not only apical but lateral lesion. You can see how the bone’s tucked back in, it’s nice and tight, and it is a regenerative procedure if properly performed. So when we do endodontics right we can grow bone. If we need an implant, this is a better site to put an implant in, even if we lost the tooth, than over here, over her on the left.
Okay, so get the splint off in about 30 days, get it out of there. Let the tooth start to function a little bit. No biting into apples, no shearing bread like a croissant or something with hard crust. Just be careful and let everything tighten up, get the splint off and there they are. So here they are at the same day, and we see a little bit of recession. That’s going to be okay because when this lady smiles we do not have a high lip line. We’re kind of like this so we’re going to be okay. But you have to talk about that before, because what if they did have a high lip line? Then you have to tell them that sometimes when we do an intentional replant there’ll be a little bit of osseous remodeling and there’ll be a little bit of gingival recession and you might show a little bit below – or above in this case – the margin of the crown.
Okay, the last case will go fast because it’s an abortion. This is an example – so I tried to give you three examples. Deficiencies in treatment aren’t considered necessarily huge errors; that’s just probably prior training. And then we talked about the iatrogenics. Nobody teaches this in dental school. Nobody talks about making an autobahn to the freeway, straight as an arrow, go as fast as you can. We have to remember, when you see this little line in here, that little black line; you see this and then you pick it up again down here. That is in a cross-section, that’s the furcation and this shape is like this. So the shape has exceeded the confines and the boundary lines of the root itself.
So I can’t do anything here. Of course apically the root’s over here, the foramen is over here, there’s two canals so I don’t know if there’s one or two. But it’s been transported and ripped here, it’s been ripped, torn and perforated furcally – that’s a stripper if you want the terminology. And then nothing there. And then here I’m thinking well, I have an infrabony pocket, I have a little furcal thing so that’s probably how the bone comes. And I’m thinking I’d better retreat this canal, because what if there’s a branch that comes off and that would explain that. So if you’re going to extract the tooth you might be able to see it; you might not be able to see it. There might be a tissue tag over it, and again you’re not going to curette the root, because by curetting the root you’re going to increase the almost 100% likelihood that the tooth will be lost through resorption.
So I’m going to go in the distal root. I’m not trying to do a Cliff Ruddle job on this; I’m just going in there to find another canal. There’s two canals. I’m not really worried about getting down around to the end of the root because the treatment plan is to remove the tooth, apicoectomy. So I just need to shape somewhat short and get a nice, tight pack, and that’s what we did.
So outside the mouth you can make these big repairs. Now you can see perfectly the concavity. That’s the concavity on the back side of that root, the distal aspect of the mesial root. And you can see we’ve got it corked apically, two systems that merged apically apparently, but they kind of diverged to go their separate ways as I prepped up the root coronally, extra orally. And there it is.
So again, this is another 10-year result. You can see the tissue, I think, piled up here if you look really carefully. But here’s the bone level, and this bone level somehow scallops back up and gets back on up to there. So I’ve got good, tight furcal bone, good tight furcal bone. I’ve got distal healing, apical healing, and that is the power, ladies and gentlemen, girls and boys, hobos and tramps. Intentional replants can be a very, very excellent choice on a strategic tooth that has the kind of root anatomy that’s conducive to an extraction. Keep it in mind and keep it on your radar.